18 The European Journal of Oriental Medicine
e erapeutic Role of the Practitioner’s
Heart in Classical Chinese Medicine
and Modern Medical Science
A critical literature review
Stéphane Espinosa
Abstract
This critical literature review focuses on the therapeutic role of
the practitioner’s heart, with emphasis on the acupuncturist’s
perspective.
The relevant descriptions given in classical Chinese medicine
are presented. In particular, the appropriate attitude of the
practitioner during treatment is discussed, highlighting the
importance of compassion and clarity of intention. This is followed
by a description of the acupuncture needle’s role of energetic link
with the patient.
Parallels were identified with results from modern research
showing that positive emotions such as compassion increase
the coherence of the cardiac electromagnetic field, and thereby
interpersonal effects such as cardiac energy exchange and
synchronisation of heart rates and heart-brain wave patterns.
The importance of these findings in providing a rationale for a
patient-centred approach to treatment is discussed, together with
the need for further research within the framework of modern
validation of classical Chinese medicine.
Key words
Heart, compassion, intention, spiritual pivot, therapeutic
relationship, acupuncture, energy exchange, biofield,
electromagnetic field, coherence, entrainment, interpersonal
effect, synchronisation.
1. Introduction
The focus of this critical literature review is on the role of the heart
in therapy, with emphasis on the acupuncturist’s perspective, as it
stems from the ancient texts of classical Chinese medicine, as well
as the modern scientific understanding of the heart.
The term ‘classical’ in the title denotes an approach that relies on
tradition and its Daoist roots, in contrast with the more modern
‘traditional Chinese medicine’ whose focus is more pragmatic,
based on scientific materialism and Confucianism (Fruehauf,
2006).
This section presents an overview of this critical literature review
and gives a brief description of the heart from the viewpoints
of classical Chinese medicine and modern medical science
respectively. This section also details the inclusion/exclusion criteria
followed in this review. Section 2 looks at the therapeutic role of
the practitioner’s Heart (心 xin) during treatment, according to
classical Chinese medicine. Section 3 reviews the modern research
on interpersonal physiological and psychological effects of the
heart’s electromagnetic (EM) field, with emphasis on their possible
therapeutic applications. Section 4 is a discussion and reflection
on the information drawn from Sections 2 and 3, in order to
determine the extent to which the knowledge acquired by ancient
Chinese therapists from their practice and intuition is supported
by using the scientific method. Finally Section 5 concludes this
critical literature review.
The Heart (心 xin) has a central importance in classical Chinese
medicine, as discussed in the early acupuncture literature (circa
200 B.C.): the Huang Di Nei Jing (黃帝內經 The Yellow Emperor’s
Classic of Internal Medicine) which is composed of the Su Wen
(素問 Essential Questions) and Ling Shu (靈樞 Spiritual Pivot) (Birch
and Felt, 1999; Lu, 2004; Unschuld, 1985).
In Su Wen chapter 8, which lists the organs, the Heart is in prime
position and is described as the emperor of the whole body (Larre
and Rochat de la Vallée, 1985). This pre-eminent position is due to
the Heart’s relationship with the shen (神), the sacred light which
illuminates the person with the spiritual aspect of the universe
and gives consciousness and discernment (Fruehauf, 2012; Larre
et al, 1986). Shen has also been translated by Maciocia (2005) as
the Mind of a person, and Spirits by Larre and Rochat de la Vallée
(1991b). Ling Shu chapter 71 states the spiritual importance of
the Heart by explaining that it is the residence of the shen (Larre
and Rochat de la Vallée, 1991a; Lu, 2004).
It is important to clarify that in the Chinese language, the
character for the Heart, 心 (xin), refers implicitly to its physical,
but also more importantly to its emotional and spiritual aspects
(Jarrett, 1998; Rochat de la Vallée, 2009; Roth, 1999). Although
it is commonly translated as Heart, xin refers to the core of
the human being. It has no flesh radical (月) which denotes
its immaterial and spiritual aspect. Its physical aspect acts as
a receptacle for the shen (Fruehauf, 2012). Chapter 18 of the
Huainan Zi (淮南子 The Masters/Philosophers of Huainan; written
circa 200 B.C. by Liu An, Prince of Huainan) says that the Heart

The European Journal of Oriental Medicine 19
e erapeutic Role of the Practitioner’s Heart in Classical Chinese Medicine and Modern Medical Science
Stéphane Espinosa
(xin) is that which from a dot extends infinitely (Robinet, 1993).
Xin is both ‘Heart’ and ‘Mind’, inextricably linked as an interactive
unit, so xin may be referred to as the compound ‘Heart-Mind’
(Birch, 2009a; Matsumoto and Birch, 1988). More generally, the
mind, energy, emotion and body are almost never distinguished
in Oriental tradition, but are viewed as a continuum (Matsumoto
and Birch, 1988). This non-dual view of mind and matter is
summarised in the Buddhist Heart Sutra as ‘form is emptiness,
emptiness is form’ (Dalai Lama, 2005: 60).
In Western medicine, until relatively recently the heart was
considered merely as a mechanical pump for blood circulation,
but is now also viewed as a neurological, endocrine and immune
organ, as discussed in detail by Pearsall (1998) and Loh (2008).
The heart’s electrical activity has been studied since the 19th
century, with the electrocardiogram (ECG) first used in 1887
to detect changes in electrical potential on the body surface
(Columbia Encyclopedia, 2012). The natural evolution of this field
of research has been to look at the human EM field (to which
the heart makes the greatest contribution) as part of biofield
physiology research (Hammerschlag, 2012; Hintz et al, 2003;
McCraty, 2003; Rubik 2002, 2005, 2008).
This critical literature review used as inclusion criteria any text (in
English, otherwise French, Spanish or Italian) that is:
• either a translation of a classic Chinese text or a modern
commentary discussing the significance of the Heart in the
Chinese medical model, as it applies to the practitioner, and in
particular to acupuncturists
• a discussion of modern research on interpersonal effects of the
heart’s EM field.
The following exclusion criteria determined the studies beyond the
scope of this review:
• untranslated Chinese texts, even if the abstract is translated
(none appeared in the literature review)
• inner cultivation of the practitioner and possible emission of qi
(for example in medical qigong training) (Chen, 2004; Johnson,
2000)
• discussions on the possible non-local effects of EM elds or
intention (Tiller, 1993)
• ‘limbic resonance’ (tuning into another’s inner emotional state)
(McTaggart, 2011)
• placebo effect (Diebschlag, 2010)
• discussions of heart pathology
• research on the effects of the heart’s EM eld within one person
(McCraty et al, 2009).
2. The therapeutic role of the practitioner’s ‘Heart-Mind’
concept in classical Chinese medicine
The consequences of connecting with the shen are discussed
as early as the Nei Ye (內業 Inward Training; possibly written in
the 5th century B.C., with unclear authorship), which predates
the Su Wen (Birch, 2009a; Roth, 1999): Through self-cultivation
one can refine one’s qi and as a result the shen (the most highly
refined form of qi) resides within the body so one benefits from
shen ming (神明 Divine Illumination) (Puett, 2002). One can then
understand the workings of the universe, and that any change is
the product of qi transformations, thereby obtaining knowledge
about, and control over other things (including humans), since
they all consist of qi (Puett, 2002) . Such a self-cultivated person
can create change without expending energy (Roth, 1999).
In the Zhen Jiu Da Cheng (针灸大成 Great Compendium of
Acupuncture and Moxibustion) compiled in 1601 by Yang
Jizhou (a doctor in the Ming dynasty, 1368-1644) and cited by
Matsumoto and Birch (1988: 38), it says that when the Mind of
the physician has a receptive and accepting attitude, without
desires, it can become shen (神).
Fruehauf (2012) explains that xin (心) is not only a receiver for
the shen, but also a transmitter of this sacred presence from the
immaterial into the material realm, so that shen ming means
making the shen visible in our immediate environment. This can
be interpreted energetically but also through the action of speech.
Indeed, xin governs the tip of the tongue, thereby expressing de
(德 Virtue) with words of wisdom (Fruehauf, 2012). De develops
with self-cultivation and is part of a healer’s training to become a
good practitioner. Besides touch and technique, the Spirit of the
physician is an important consideration in therapy (Matsumoto
and Birch, 1988). In other words, the practitioner may illuminate
the patient with their shen ming energetically as well as with
wise speech.
2.1. Physician attitude
Sun Simiao’s (581-682 A.D.) writings, translated by Unschuld
(1979), advise that during treatment, a great physician has to
be mentally calm and their disposition firm, without wishes or
desires. They have to develop an attitude of compassion and be
willing to make the effort to save every living creature. This echoes
sections 27 and 67 of the Dao De Jing (道德經 The Classic of
the Way and the Virtue; possibly written in the 5th century B.C.
originally by the legendary Lao Zi), which explain that the sage
(who lives according to the Dao) considers their compassion as a
treasure and always helps and rescues living creatures. It would
therefore be beneficial for an acupuncturist to take the sage as
model (Strom, 2004).
When the practitioner’s own Heart is still, trust is established
and contact can be made with the truth in the patient’s Heart.
The healer does not impose their will, but assists patients in
transforming by themselves (Jarrett, 1998). For this to occur, the
appropriate conduct in clinic (and more generally in everyday life)
is obtained by the practice of xin shu (心術 The Art of the Heart)
which cultivates serenity and leads to xin xu (心虚 The Void of the
Heart) where knowledge becomes wisdom (Rochat de la Vallée,
2009).
A different aspect of the practitioner’s appropriate attitude is
described in Su Wen chapter 25 and chapter 54: the hand holding
the needle should be manoeuvred with great concentration and
strength, as if holding a tiger. The acupuncturist should remain
as alert and careful as if being at the edge of an abyss, and they
must rectify their own shen in order to rectify the shen of the
patient (Lu, 2004; Rossi, 2007). This is echoed in Ling Shu chapter

20 The European Journal of Oriental Medicine
9, which explains that while needling, the physician should remain
only attentive to the act of needling, and nothing else, as if being
in a remote place for contemplation (Lu, 2004).
While treating, a practitioner should have a clear intention (by
focusing on the therapeutic function of acupuncture points)
otherwise the effect of their needling will convey an unclear
treatment strategy with unclear results (Yuen, 2005). Clarity of
intention is also brought by alignment with the shen, as discussed
in the following section.
2.2. Spiritual connection with the outside world
Guo Yuzeng (a doctor in the Eastern Han dynasty, 25-220), cited
by Lu (2004: 402) in his translation of the Ling Shu chapter 8, says
that the Spirit is in between the physician’s Heart and their hand.
Thus, acupuncture treatment should be focused on the Spirit,
including the Spirit of the patient and that of the acupuncturist.
The practitioner’s own internal alignment with Heaven (spiritual
development and cultivation of Virtue) is responsible for successful
treatment because it creates a context for healing even before the
needles are inserted (Jarrett, 1998).
During treatment, the practitioner’s ability to use their intention,
the quality of their presence or attention, are as important as the
points selected or the stimulation provided. In other words, the
practitioner may use their qi for further influencing a change in
the patient’s qi (Schnyer et al, 2008).
Furthermore, through the power of their intention, the
practitioner can direct the energies controlled by acupuncture
points. However, the practitioner must understand clearly and
consistently what they intend the points to do if their intention is
to be communicated to the patient’s energy (Pirog, 1996).
Yi (意) refers to intention, without a specific goal or plan for its
realisation, as opposed to thoughts actively translated into
action, which are zhi (志), the Will (Matsumoto and Birch,
1988). With the yi, the practitioner extends their awareness of
the surrounding energy. In addition, their intention and focus
on a selected treatment strategy depend on the clarity of their
connection with the shen (Houghton, 2010). The importance
of this in clinic is that acupuncture points often have several
functions and consequently different effects depending on
the practitioner’s focus and school of thought. In addition,
Gardner-Abbate (1996) describes how a given point function
may have different applications: for example, luo-Connecting
and yuan-Source points of coupled meridians can be used in
combinations or needling styles that are different in the English
or Chinese traditions, to either tonify or disperse the energy of
a meridian (and associated organ), yet clinically those different
strategies work.
The practitioner’s intention is also discussed by Hammer (1990)
who points out the similarity between psychology and Chinese
medicine: the healer is a significant factor in the healing process.
Their intention (both the conscious and the unconscious) and their
life-force are energies capable of profoundly interacting with the
energies of the patient, even influencing them for better or
worse (Hammer, 1990). Lawson-Wood (1973) cited by Hammer
(1990) also states that the practitioner’s Mind, their intention,
has great influence upon the quality of the treatment that they
will administer.
Hammer (1990) stresses the fact that the physician remains
objective in their diagnosis, in particular via the art of observation
of phenomena, but not alienated (such as Western physicians may
be due to the lack of training of their senses and a cultural bias
in favour of ‘professional distance’). Together with needles and
herbs, their energy is accepted as a meaningful part of the healing
process. In particular, when the practitioner lays hands on the
patient, in terms of healing, there is the transmission of the sense
of caring, which is a form of love. Love is ultimately the great
healer, and in such a relationship the physician and patient are
mutually nourished (Hammer, 1990).
Finally, Fruehauf (2012) gives a poetic description of xin as being
a central altar with the functions of connecting with the shen, but
also establishing and maintaining unity (through the act
of connection of the micro and macrocosms) and community
(by connection to a higher nature).
2.3. Spiritual pivot
Birch (2009a) reviewed the translations of Ling Shu chapter 1,
where it is said that the shen or the Mind (the Heart being of
course the link between the two translations) of the practitioner
should focus at the needle tip for effective needling, which implies
an effect of the Mind on the qi.
In their commentary of Ling Shu chapter 8, Larre and Rochat de
la Vallée (1991b) explain that the needle can be like a pivot that
establishes communication so that the influences of Heaven (the
spiritual aspect of life) can penetrate the patient. The Spirits, shen,
are like messengers, carrying the influence of Heaven, so they
are an intermediary between Heaven and Man, and the centre
of reception of these influences is the void of xin, the Heart-
Mind. Firebrace (1993), cited by Blackwell et al (1993), says that
the practitioner should have good shen ming (Radiance of the
Spirit), as a catalyst in treatment (and for their own preservation),
although the acupuncture treatment works of itself, using the
needle as a ‘ling shu’, a Spiritual Pivot. Larre and Rochat de la
Vallée (1991b) then suggest that the shen can pass between
the physician and the patient, or the physician himself is just
a pivot like the needle to re-establish an equilibrium that has
been disturbed.
The Zhen Jiu Da Cheng (mentioned above), cited by Matsumoto
and Birch (1988: 38), explains that the xin of the physician and the
patient should be level and in harmony, following the movements
of the needle. Consequently, the acupuncturist, patient and needle
form a synergetic unit so that the healing process goes beyond the
mere fact of needling (White et al, 2008). Indeed, for an effective
treatment, the acupuncturist goes all the way to the origin of the
patient’s life, to the place where the Spirits are rooted in order to
attract them so that they bring forth the Heavenly influence in the
patient (Larre and Rochat de la Vallée, 1992, 1995).
The European Journal of Oriental Medicine 21
3. Review of research on interpersonal effects of the human
heart EM field
3.1. Cardiac energy exchange
The heart generates the strongest EM field of the body (up to
100 times stronger than that produced by the brain) and can
be measured meters away from the body (McCraty et al, 1998;
McCraty et al, 2012). Pearsall (1998) concurs by stating that when
the heart beats, it generates energy that is not contained within
us, and thereby may be able to signal other hearts. Moreover,
cellular regulation can be influenced by EM fields pulsing in the
same frequency range as the cardiac field, hence it is possible that
a practitioner’s heart has a therapeutic effect by influencing the
patient via its radiated EM field (Oschman, 2003).
This is of particular relevance because the lack of a plausible
mechanism to explain the nature of an energy exchange between
people, or how it could affect or facilitate the healing process,
causes a major block for its acceptance by Western science
(McCraty et al, 1998). Consequently, the possibility of people
exchanging energy via the heart EM field was investigated by
Russek and Schwartz (1994) as well as McCraty et al (1998).
The first step was to consider how an external EM field may
affect biological systems, given that the EM field radiated by
the human heart was theoretically calculated to be too weak
(Weaver and Astumian, 1990). The proposed underlying
mechanisms were cellular signal averaging (where the cell’s
membrane averages the EM field, which reduces the noise –
random fluctuating thermal energy) and stochastic resonance
(where the noise within a biological system is entrained by an
external periodic signal – here the cardiac EM wave – thereby
increasing the signal intensity up to a level where it can interact
with the system) (McCraty, 2003).
Both groups independently demonstrated that when people
touch or are in proximity, the ECG signal of one person (the
‘source’) is registered in another person (the ‘receiver’) on the
body surface (including in the electroencephalogram (EEG)), hence
showing an exchange of EM energy produced by the human
heart (McTaggart, 2008). This occurred in both directions (the two
persons affecting each other: the other’s ECG signal detected in
one’s EEG) in about 30 per cent of the subject pairs, otherwise
only in one direction, indicating a varying degree of signal
transmission. Indeed, Russek and Schwartz (1994) determined
that people more accustomed to receiving love and care appear
to be better receivers of others’ cardiac signals, and therefore
this energy exchange plays an important role in empathy and
sensitivity to others (McCraty, 2003).
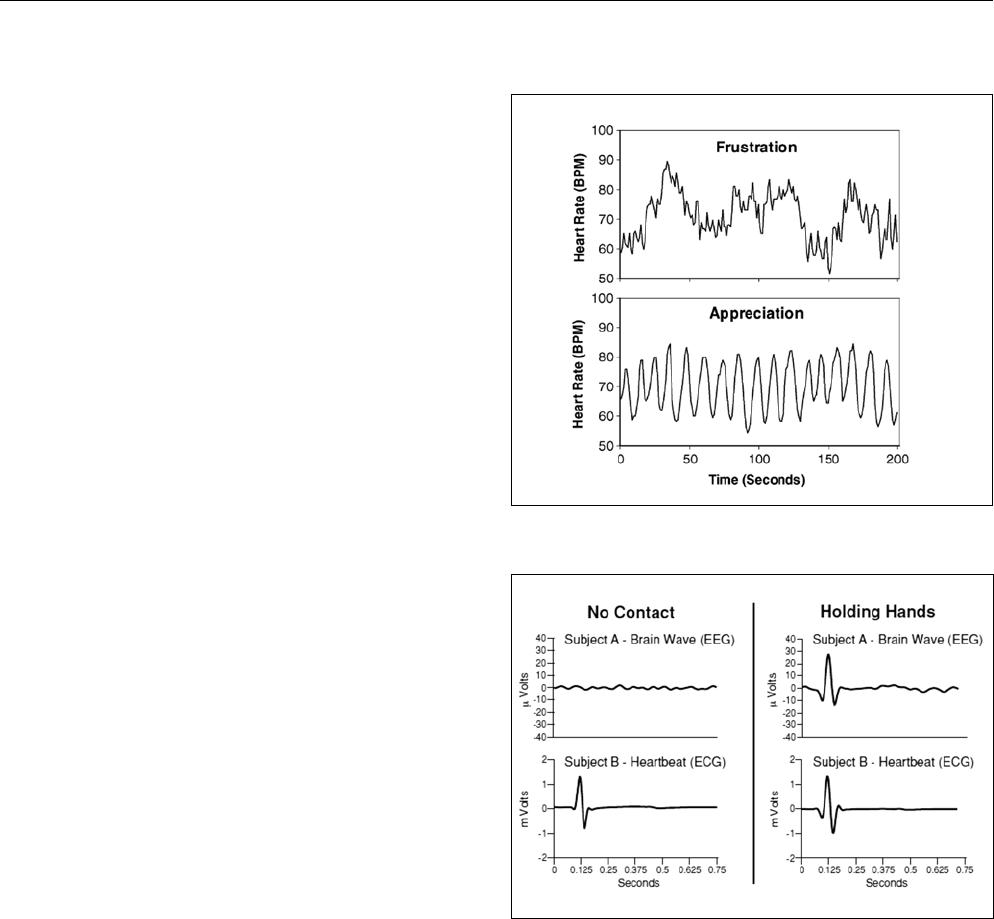
In addition, when a person feels a positive emotion (such as
sincere love or appreciation) or has a caring intention, this
increases coherence (the periodic nature) in the cardiac rhythm
(and hence in the EM field), providing various health benefits,
such as higher immunity, reduced hypertension or emotional
disorders; by contrast, a negative emotion is associated with a
more erratic pattern, as shown in figure 1 (McCraty et al, 2009;
Rosch, 2009; Tiller, 1990).
Figure 1: Emotions are reflected in heart rhythm patterns
(McCraty et al, 2009: 22).
Figure 2: The electricity of touch, heartbeat signal averaged
waveforms
(McCraty, 2003: 9)
In other words, in these circumstances clearer information is being
transmitted outside of the body. This prompted McCraty et al
(1998) to propose that via the mechanism of stochastic resonance,
this increased coherence may improve the cardiac energy
exchange between people. In particular, the nervous system may
act as an antenna, responding to the EM fields produced by the
hearts of other people (McCraty, 2003; McCraty et al, 2005).
In their experiments, McCraty et al (1998) did not instruct their
subjects to have any specific intention or feeling state (presumably in
order to introduce fewer variables in the initial study). The transfer of
cardiac energy was detected when the subjects were holding hands
(or in close proximity – about 45cm) as shown on the right side of
figure 2, but not when separated by one meter (figure 2 left side). In
figure 2, the source and receiver are subjects B and A, respectively (no
difference was found between genders) (McCraty, 2003).
e erapeutic Role of the Practitioner’s Heart in Classical Chinese Medicine and Modern Medical Science
Stéphane Espinosa

22 The European Journal of Oriental Medicine
However, Russek and Schwartz (1994) did observe in their
preliminary results the energy exchange between people (heart-
brain and heart-heart) for a distance between subjects of up to
one meter, with their eyes closed and not communicating in any
tactile, visual, or auditory way. This discrepancy in detections is
possibly due to the reasons stated above (variability of source
and receiver) as well as duration of observation time (affecting
the averaging of the signal and thereby the noise level). Finally,
by comparing the amplitude of the transferred signal observed in
hand holding and non-contact trials (tenfold amplitude reduction
in the latter type, with distance taken into account), McCraty et
al (1998) concluded that electrical conduction (through direct skin
contact) plays a bigger role than EM radiation. (For completeness,
McCraty (2003) mentioned that instead of a radiated wave, the
signal may be transferred by electrical capacitive coupling due
to the potential difference between individuals). In any case,
this observed cardiac energy exchange represents a plausible
mechanism for how one person can sense the presence of
another and even their emotional state, independent of other
signals such as body language (McCraty et al, 2009).
Morris (2010) then researched ‘collective coherence’, that is
whether a group of people trained in achieving a high state
of coherent cardiac field (focusing on the heart rate variability)
could facilitate coherence in an untrained person. Using 15
trained ‘senders’ and as many non-trained ‘receivers’, the study
comprised a series of 148 10-minute trials. Each session consisted
of a receiver seated in close proximity to three senders who were
instructed to alternatively direct toward the receiver their focused
care and compassion, or focus on their coherence technique with
no attention directed to the receiver.
Due to the wide variability in the receivers’ achieved coherence,
significant differences were difficult to establish, so a matched
comparison analysis was conducted, showing that receivers
obtained a higher coherence in 47.3 per cent of the cases.
Another result was that when senders focused on achieving
high coherence themselves, it better helped in raising the
receiver’s coherence than when attempting to facilitate the
process. Morris (2010) interpreted this finding as indicating that
the act of trying to direct facilitative energy may actually interfere
with energetic transfers.
Morris (2010) then explained that the study design had assumed
that senders could influence the receiver’s cardiac field unilaterally.
However, the sender-receiver circuit appears in fact to be a
dynamic two-way channel, possibly influenced by either party. By
asking participants how they felt about each other, Morris (2010)
determined that the quality and extent of their interpersonal
relationships had a greater effect on any energetic interaction,
than the actions and intentions of the senders.
3.2. Interpersonal heart-brain synchronisation
In further non-contact trials, McCraty (2003) separated the
subjects by one and a half meters and asked them to maintain a
positive emotional state (although no specific intention to send
energy) in order to produce a sustained coherent cardiac EM field.
McCraty (2003) showed that the receiver’s alpha waves rhythm
(one type of the brain’s oscillating electrical voltages) synchronised
with the source’s ECG pattern, but only if the receiver maintained
a coherent field, which could be the reason for being more
sensitive to others’ cardiac signals, as discussed above (Russek
and Schwartz, 1994; Tiller, 1990). McCraty (2003) highlighted
the importance of this interpersonal non-contact heart-brain
synchronisation, as it may play a role in the non-verbal aspect
of therapeutic interactions (by promoting greater rapport and
empathy). However, he did not elaborate on the significance
of the synchronisation occurring with this particular type of
brain wave. Oschman (2000) also conjectured that the source’s
radiated EM field may have healing power thanks to its ability
to entrain (synchronise) similar coherent rhythms in the tissues
of the receiver.
The results by McCraty (2003), McCraty et al (1998) and Russek
and Schwartz (1994) reported in sections 3.1 and 3.2 were from
selected representative examples to be considered as a proof of
concept rather than be subjected to statistical analysis. There
was no discussion of the level of blinding selected and whether
randomization was used.
3.3. Interpersonal heart-heart synchronisation
McCraty (2003) also reported anecdotal evidence of heart rhythm
entrainment (synchronisation) between individuals having a close
relationship and while they focused on generating feelings of
appreciation for each other. Subjects were separated by about one
meter. Intermittent heart rate synchronisation was also observed
during sleep in couples who are in long-term stable and loving
relationships (McCraty 2003).
Subsequently and independently, Bair (2006, 2008) conducted
research on the heart rate synchronization between a healer
having a positive intent and a subject. The total sample size
was 91 adults, of which 41 comprised the control group. All
participants came for a one-hour treatment and during the
session were taught how to apply a self-relaxation technique,
while being kept blind to the study’s actual focus. Pulse and
respiration were checked before and after the session. The healer
was presented as a researcher and met the whole control group
together for one hour, remained more than six meters away from
participants and without specific intention. The healer then met
individual members of the intervention population for one hour,
and sat within one and a half meters of the participant (distance
determined from McCraty’s (2003) results), focusing on a heart
connection of compassion and highest good.
Bair (2006) found that the healer effect was visible in the
synchronisation of healer/subject heart rates in the intervention
subjects (which did not occur in the control subjects). Whereas
before the session there was no significant correlation, just after
the treatment 60 per cent of the intervention population had
heart rates within ±2 beats per minute of the healer’s. Pearson’s r
analysis (a measure of correlation) on the healer and subject heart

The European Journal of Oriental Medicine 23
rates was .671 (P ≤.001 hence statistically significant) indicating a
strong correlation. The healer effect was also apparent in a higher
degree of reported (hence subjective) health improvements in the
intervention population (reduced level of distress concerning the
issue for which they had the treatment).
Bair (2008) explained that heart rate synchronisation implies
a resonance entrainment (made possible due to the healer’s
cardiac EM field being coherent), with the possibility of transfer
of information or regulation between healer and subject
(corroborated by the reported health improvement), although it
may occur on an energy level below the threshold of conscious
awareness.
Morris (2010) also observed heart rate synchronisation between
participants in his ‘collective coherence’ study (section 3.1), with
870 inter-subject heart rate observations in total. Of the subject
pairs, 37.9 per cent showed a correlation statistically significant
from zero (Pearson’s r > .062 at P ≤.05, given the large number
of data: 2400 samples in a ten-minute time series). Interestingly,
higher levels of heart rate synchronisation were found to be
correlated with higher coherence levels (of heart rate variability).
4. Discussion
Schnyer et al (2008) suggested that there is a form of
physiological concordance in the patient-practitioner interaction.
They proposed that there is a relationship between simultaneous
changes in physiological measures (such as heart rate, skin
conductance, blood pressure, respiratory rate, etc.) between
the patient and practitioner, which enables access to the
signalling system activated by acupuncture. They also stated that
experimental evidence is not yet present.
However, in view of section 3, modern research has started
providing such evidence. McCraty (2003) explained that a clinician
with heartfelt positive emotions and attitudes will have a more
coherent cardiac field (to which the patient is exposed), which
may enhance the non-verbal aspect of the therapeutic interaction,
and possibly also positively affect the patient’s physiology and
receptivity to treatment. This last statement has started to be
researched by Bair (2006), who reported results of reduced
levels of distress (see section 3.3), implying that more than just
synchronization is happening.
Also, as Birch (2009b) pointed out, since an acupuncture
treatment involves touch of the patient by the practitioner, the
cardiac energy exchange does occur and may trigger changes in
the patient’s EM field (via the EM fields of the heart and brain).
The effect would be to induce or enhance beneficial physiological
effects produced by an increase in the patient’s cardiac field
coherence. This modern view of linkage by a coherent cardiac
field parallels the 17th century recommendation given in the Zhen
Jiu Da Cheng (mentioned in section 2.3), cited by Matsumoto and
Birch (1988: 38), that the xin (the Heart-Mind) of the physician
and the patient should be level and in harmony, following the
movements of the needle.
Interestingly, the needles used in acupuncture are metallic, and
as such they conduct electricity while being affected by the
surrounding EM field. When a needle is inserted at the location of
an acupuncture point, it will affect the electrical current flowing in
the corresponding meridian (Becker and Selden, 1985). Hence the
effect of the practitioner’s coherent cardiac field on the patient
may be focused by the needle. This idea resonates with the
concept of ‘ling shu’ (detailed in section 2.3), the Pivot passing
the shen between practitioner and patient.
In both classical Chinese and modern approaches, the
practitioner’s intention or mental focus is an important
factor modulating the effect of the heart. Indeed, a healer’s
compassionate intent can cause interpersonal non-contact
synchronisation of heart and brain, as shown by McCraty (2003)
(section 3.2), as well as heart rates (Bair 2006) (section 3.3).
Morris (2010) also observed heart rate synchronisation in his
‘collective coherence’ study (section 3.1), opening up the
possibility for what he calls ‘heart-to-heart bio-communications’
(Morris 2010: 72). Therefore practising emotional empathy
is mutually beneficial, as thoughts and emotions are likely to
influence the qualitative aspects of the energetic interactions
between people. This is consistent with Pearsall (1998) who
proposes that a patient is healed by the presence of ‘healing
loving hearts’ joining with their heart, and not just by the actions
of medical staff. However, Morris (2010) explained that, based on
his results, it is best not to try to impose a particular emotional
state on others, as energetic interactions seem to be impeded
rather than enhanced when over-engaging the mind relative to
the heart. In other words, personal coherence seems to be the
best foundation to forge collective coherence. This is supported by
the results of a large-scale sociological project (5,124 participants)
using data of the Framingham Heart Study: a happy next-door
neighbour increases one’s probability of happiness by 34 per
cent, and a happy friend living within a mile by 25 per cent
(this effect decays with time and geographical separation). This
implies that happiness, like health, should be seen as a collective
phenomenon, since people’s happiness depends on the happiness
of others with whom they are connected (Fowler and Christakis,
2008; McTaggart, 2011).
5. Conclusion
The recent research findings from McCraty et al (1998, 2005,
2009), Russek and Schwartz (1994), Bair (2006) and Morris (2010)
indicate that the practitioner’s heart plays a role in the healing
encounter. In particular, the observed cardiac energy exchange
and interpersonal synchronisation parallel the classical Chinese
medical descriptions of the physician’s appropriate behaviour
and the acupuncture needle acting as a link and focus of energy
passing to the patient. These preliminary results warrant further
research: a comprehensive rigorous study of these elements of
convergence, which may provide a basis for further modern
validation of classical Chinese medicine, and thereby a greater
public acceptance.
e erapeutic Role of the Practitioner’s Heart in Classical Chinese Medicine and Modern Medical Science
Stéphane Espinosa

24 The European Journal of Oriental Medicine
This research should eventually benefit the patients’ health, hence
the increasing interest on this topic, with gradually more Western
doctors asking whether the subtle bioelectromagnetic energy can
be harnessed for health enhancement (Rosch 2009). The results
reported in this review already show the importance of a patient-
centred rather than a disease-centred approach to treatment
(Jones 2010). In other words, Western-trained clinicians should
evolve from the role of ‘curing disease through modern science’
and back to their traditional role of ‘healer of the sick’, forming a
‘healing partnership’ with the patient (Jones et al, 2010: 72).
This has started to be considered carefully, for example by Miller
et al (2009) who characterized the placebo effect as a form of
interpersonal healing, instead of being an umbrella term for every
non-understood effect (such as EM field, beliefs or relationships)
(Diebschlag, 1993). Hence the cultivation of the practitioner’s
intention has important implications for treatment, as it enhances
both clarity of intention and the capacity to maintain energetic
coherence despite the patient’s influence (Diebschlag, 2010).
Finally, during an acupuncture treatment, the therapeutic
relationship has both specific and non-specific aspects. Rapport
building with compassion (increasing cardiac coherence) and
communication to engender empathy might be seen as non-
specific. Yet at least the two following aspects are specific to
acupuncture: 1. The fact that the needle acts as a pivot to focus
the practitioner’s intention; 2. Palpatory diagnosis to identify
points may have a therapeutically active component (MacPherson
et al, 2006; Schnyer et al, 2008; White et al, 2008). Both aspects
are consistent with the observations of cardiac energy transfer
being greater when people are in direct contact and highlight
the therapeutic role of the practitioner’s heart.
Acknowledgements
This article formed part of a BSc project for the International
College of Oriental Medicine, validated by the University of
Greenwich. Special thanks go to Francesca Diebschlag for her
thoughtful comments.
References
Bair, C. C. (2006). The heart field effect: Synchronization of healer-subject
heart rates in energy therapy Holos University (online) last accessed
02.03.2013 at http://holosuniversity.net/pdf/bairDissertation.pdf
Bair, C. C. (2008). The heart field effect: Synchronization of healer-subject
heart rates in energy therapy. Advances In Mind-Body Medicine, 23 (4),
10-19.
Becker, R. O. and Selden, G. (1985). The Body Electric: Electromagnetism
and the Foundation of Life. New York: Harper.
Birch, S. (2009). Filling the Whole in Acupuncture Part 1:1 What are we
doing in the supplementation needle technique? European Journal of
Oriental Medicine, 6 (2), 25-35.
Birch, S. (2009b). Filling the Whole in Acupuncture Part 1:2 What are we
doing in the supplementation needle technique? Scientific perspectives.
The European Journal of Oriental Medicine, 6 (3), 18-27.
Birch, S. and Felt, R. (1999). Understanding Acupuncture. London:
Churchill Livingstone.
Blackwell, R., De Soriano, G., Firebrace, P., Royds, R., Rusher, R. and
Uddin, J. (1993). The Spirit: Some Practitioner Viewpoints. The European
Journal of Oriental Medicine, 1 (1), 19-24.
Chen, K. W. (2004). An Analytic Review of Studies on Measuring Effects of
External Qi in China. Alternative Therapies in Health and Medicine, 10 (4),
38-50 (online) last accessed 02.03.2013 at http://qigonginstitute.org/html/
Chen/Waiqianalysis_0704.pdf
Columbia Encyclopedia (2012) Electrocardiography in The Columbia
Electronic Encyclopedia 6th edition, Columbia University Press (online) last
accessed 02.03.2013 at http://www.encyclopedia.com/doc/1E1-electroca.
html
Dalai Lama. (2005). Essence of the Heart Sutra: The Dalai Lama’s Heart of
Wisdom Teachings. US: Wisdom Publications.
Diebschlag, F. (1993). Placebo Acupuncture. University of Exeter.
Diebschlag, F. (2010). The Therapeutic Relationship: A Workbook for the
Healing Professions. Francesca Diebschlag (Standard Copyright Licence).
Fowler, J. H. and Christakis, N. A. (2008). Dynamic spread of happiness
in a large social network: longitudinal analysis over 20 years in the
Framingham Heart Study. British Medical Journal, 337, a2338 (online) last
accessed 02.03.2013 at http://www.readcube.com/articles/10.1136/bmj.
a2338
Fruehauf, H. (2006). Classical Chinese Medicine vs Traditional Chinese
Medicine. Holisticwebs.com (online) last accessed 02.03.2013 at http://
www.qiwithoutborders.org/classical-TCM.html
Fruehauf, H. (2012). The Organ Networks of Chinese Medicine: Heart.
Classical Chinese Medicine organisation (online) last accessed 02.03.2013
at http://www.classicalchinesemedicine.org/af/av/cosmo/organ-networks-
heart/
Gardner-Abbate, S. (1996). Holding the Tiger’s Tail: An acupuncture
techniques manual in the treatment of disease. Santa Fe: Southwest
Acupuncture College Press.
Hammer, L. I. (1990). Dragon Rises, Red Bird Flies: Psychology and
Chinese Medicine. The Aquarian Press.
Hammerschlag, R. (2012). Biofield Physiology: Exploring Interfaces
between Biofield Healing and Conventional Physiology. 14th Annual
Research Symposium. Acupuncture Research Resource Centre (online)
last accessed 02.03.2013 at http://arrcsymposium.org.uk/dr-richard-
hammerschlag-biofield-physiology-exploring-interfaces-between-biofield-
healing-and-conventional-physiology.html
Hintz, K. J., Yount, G. L., Kadar, I., Schwartz, G., Hammerschlag,
R. and Lin, S. (2003). BioEnergy Definitions and Research Guidelines.
Alternative Therapies in Health and Medicine 9 (3), 13-30 (online) last
accessed 02.03.2013 at http://mindbodylab.bio.uci.edu/publications/
Bio%20Def%20and%20Research%20Guidelines.pdf
Houghton, J. (2010). To elucidate the role of Yi Shi 意識 within the
practice of Acupuncture. International College of Oriental Medicine.
Jarrett, L. S. (1998). Nourishing Destiny, the Inner Tradition of Chinese
Medicine. Massachusetts, USA: Spirit Path Press.
Johnson, J. A. (2000). Chinese Medical Qigong Therapy: A
Comprehensive Clinical Text. The International Institute of Medical
Qigong.
Jones, D. S. (2010). Needed: A coherent architecture for 21st century
clinical practice and medical education. Alternative Therapies in Health
and Medicine, 16 (4), 64-67 (online) last accessed 02.03.2013 at http://
www.heartmath.org/templates/ihm/downloads/pdf/research/publications/
coherent-architecture-for-21st-century.pdf
Jones, D. S., Hofmann, L. and Quinn, S. (2010). 21st Century
Medicine: A New Model for Medical Education and Practice. The Institute
for Functional Medicine (online) last accessed 02.03.2013 at http://www.
functionalmedicine.org/listing_detail.aspx?id=2337&cid=0
Larre, C. and Rochat de la Vallée, E. (1985). Huang Di Nei Jing Su Wen
Chapter 8: The Secret Treatise of the Spiritual Orchid. British Register of
Oriental Medicine.

The European Journal of Oriental Medicine 25
Larre, C. and Rochat de la Vallée, E. (1991a). Aspects of the Heart.
Review of Oriental Medicine 9, 6-9.
Larre, C. and Rochat de la Vallée, E. (1991b). The Heart in Lingshu
Chapter 8. London: Monkey Press.
Larre, C. and Rochat de la Vallée, E. (1992). Les mouvements du coeur:
Psychologie des Chinois. Paris: Desclée de Brouwer.
Larre, C. and Rochat de la Vallée, E. (1995). Rooted in Spirit: The Heart
of Chinese Medicine. New York: Station Hill Press.
Larre, C., Schatz, J. and Rochat de la Vallée, E. (1986). Survey of
Traditional Chinese Medicine. Paris: Institut Ricci.
Loh, R. (2008). Views of the Heart: Parallels and divergences between
Chinese and Western perspectives of the heart. A literature review.
International College of Oriental Medicine.
Lu, H. C. (Trans.) (2004). A Complete Translation of the Yellow Emperor’s
Classics of Internal Medicine and the Difficult Classic (Nei-Jing and Nan-
Jing). International College of Traditional Chinese Medicine of Vancouver.
Maciocia, G. (2005). The Foundations of Chinese Medicine, A
Comprehensive Text for Acupuncturists and Herbalists 2nd edition.
Edinburgh: Elsevier.
Matsumoto, K. and Birch, S. (1988). Hara Diagnosis: Reflections on the
Sea. Massachusetts, USA: Paradigm Publications.
MacPherson, H., Thorpe, L. and Thomas, K. (2006). Beyond
Needling – Therapeutic Processes in Acupuncture Care: A Qualitative
Study Nested Within a Low-Back Pain Trial. The Journal of Alternative
and Complementary Medicine, 12 (9), 873-880 (online) last accessed
02.03.2013 at http://web.ebscohost.com/ehost/detail?vid=5&sid=ff8007ca-
2744-4335-a7b8-9187df46df1c%40sessionmgr13&hid=28&bdata=JnNpd
GU9ZWhvc3QtbGl2ZQ%3d%3d#db=aph&AN=23122026
McCraty, R. (2003). The Energetic Heart, Bioelectromagnetic Interactions
Within and Between People. Institute of HeartMath.
McCraty, R., Atkinson, M., Tomasino, D. and Tiller, W. A. (1998).
The Electricity of Touch: Detection and measurement of cardiac energy
exchange between people in Pribram, K. H. (ed.). Brain and Values: Is
a Biological Science of Values Possible Lawrence. Erlbaum Associates
Publishers (online) last accessed 02.03.2013 at http://www.heartmath.org/
research/research-publications/electricity-of-touch.html
McCraty. R., Atkinson, M., Tomasino, D. and Bradley, R. T. (2009). The
Coherent Heart: Heart–Brain Interactions, Psychophysiological Coherence,
and the Emergence of System-Wide Order. Integral Review 5 (2), 10-115
(online) last accessed 02.03.2013 at http://integral-review.org/back_issues/
backissue9/index.asp
McCraty, R., Bradley, R. T. and Tomasino, D. (2005). The Resonant
Heart. Shift: At the Frontiers of Consciousness 5, 15-19 (online) last
accessed 02.03.2013 at http://noetic.org/library/magazines/shift-issue-5/2/
McCraty, R., Deyhle, A. and Childre, D. (2012). The Global Coherence
Initiative: Creating a Coherent Planetary Standing Wave. Global Advances
in Health and Medicine, 1 (1), 64-77 (online) last accessed 02.03.2013 at
http://www.heartmath.org/research/research-publications/gci-creating-a-
coherent-planetary-standing-wave.html
McTaggart, L. (2008). The Intention Experiment: Use Your Thoughts to
Change the World. London: Harper Element.
McTaggart, L. (2011). The Bond: Connecting through the space between
us. Hay House UK.
Miller, F. G., Colloca, L. and Kaptchuk, T. J. (2009). The Placebo Effect,
illness and interpersonal healing. Perspectives in Biology and Medicine, 52
(4), 518-39 (online) last accessed 02.03.2013 at http://tedkaptchuk.com/
selected-publications
Morris, S. M. (2010). Achieving collective coherence: Group effects
on heart rate variability coherence and heart rhythm synchronization.
Alternative Therapies in Health and Medicine, 16 (4), 62-72 (online)
last accessed 02.03.2013 at http://www.heartmath.org/templates/ihm/
downloads/pdf/research/publications/achieving-collective-coherence.pdf
Oschman, J. L. (2000). Energy Medicine: The Scientific Basis. Elsevier.
Oschman, J. L. (2003). Energy Medicine in Therapeutics and Human
Performance. Elsevier.
Pearsall, P. (1998). The Heart’s Code: Tapping the Wisdom and Power of
Our Heart Energy. New York: Broadway Books.
Pirog, J. E. (1996). The Practical Application of Meridian Style
Acupuncture. California, USA: Pacific View Press.
Puett, M. J. (2002). To Become a God: Cosmology, Sacrifice, and Self-
Divinization in Early China. Massachusetts, USA: Harvard University Press.
Robinet, I. (Trans.) (1993). Traduction du dix-huitieme chapitre: Parmis
les hommes in Larre, C., Robinet, I. and Rochat de la Vallée, E. (eds.). Les
grands traits du Huainan zi. Paris: Les Editions du Cerf.
Rochat de la Vallée, E. (2009). Les 101 Notions-Clés de la Médecine
Chinoise, 2nd edition. Paris: Guy Trédaniel Editeur.
Rosch, P. J. (2009). Bioelectromagnetic and Subtle Energy Medicine: The
Interface between Mind and Matter. Annals of the New York Academy of
Sciences, 1172, 297-311 (online) last accessed 02.03.2013 at http://www.
methodesurrender.fr/docs/art_bsem_2009.pdf
Rossi, E. (2007). Shen: Psycho-Emotional Aspects of Chinese Medicine.
Edinburgh: Elsevier.
Roth, H. D. (1999). Original Tao: Inward Training (Nei Yeh) and the
Foundations of Taoist Mysticism. New York: Columbia University Press.
Rubik, B. (2002). The Biofield Hypothesis: Its Biophysical Basis and Role in
Medicine. The Journal of Alternative and Complementary Medicine, 8 (6),
703-717 (online) last accessed 02.03.2013 at http://web.ebscohost.com/
ehost/pdfviewer/pdfviewer?sid=06fa9a55-b62e-4a20-ba42-95adfff4ed33
%40sessionmgr115&vid=2&hid=105
Rubik, B. (2005). The Flame of Life. Shift: At the Frontiers of
Consciousness, 5, 20-24 (online) last accessed 02.03.2013 at http://noetic.
org/library/magazines/shift-issue-5/3/
Rubik, B. (2008). Measurement of the Human Biofield and Other Energetic
Instruments in Freeman, L. (ed) Mosby’s Complementary & Alternative
Medicine: A Research-Based Approach: A Research-based Approach.
Mosby Elsevier (online) last accessed 02.03.2013 at http://www.faim.org/
energymedicine/measurement-human-biofield.html
Russek, L. G. and Schwartz, G. E. (1994). Interpersonal Heart-Brain
Registration and the Perception of Parental Love: A 42 Year Follow-Up of
the Harvard Mastery of Stress Study. Subtle Energies, 5 (3), 195-208.
Schnyer, R. N., Birch, S. and MacPherson, H. (2008). Acupuncture
practice as the foundation for clinical evaluation in MacPherson, H.,
Hammerschlag, R., Lewith, G. and Schnyer, R. N. (eds.) Acupuncture
Research, Strategies for Establishing an Evidence Base. Edinburgh: Elsevier.
Strom, H. (Trans.) (2004). Livre de la Voie et de la Vertu: Laozi – Dao De
Jing à l’usage des acupuncteurs. Paris: Edition You Feng.
Tiller, W. A. (1990). A Gas Discharge Device for Investigating Focussed
Human Attention. Journal of Scientific Exploration, 4 (2), 255-271 (online)
last accessed 02.03.2013 at http://www.scientificexploration.org/journal/
jse_04_2_tiller.pdf
Tiller, W. A. (1993). What are subtle energies? Journal of Scientific
Exploration, 7 (3), 293-304 (online) last accessed 02.03.2013 at http://
www.scientificexploration.org/journal/jse_07_3_tiller.pdf
Unschuld, P. U. (1979). Medical Ethics in Imperial China: A Study in
Historical Anthropology. Berkeley: University of California Press.
Unschuld, P. U. (1985). Medicine in China: A History of Ideas. Berkeley:
University of California Press.
Weaver, J. C. and Astumian, R. D. (1990). The response of living cells
to very weak electric fields: The thermal noise limit. Science, 247, 459-
462 (online) last accessed 02.03.2013 at http://www.highbeam.com/
doc/1G1-8533713.html
White, P., Linde, K. and Schnyer, R. N. (2008). Investigating the
components of acupuncture treatment in MacPherson, H., Hammerschlag,
R., Lewith, G. and Schnyer, R. N. (eds.) Acupuncture Research, Strategies
for Establishing an Evidence Base. Edinburgh: Elsevier.
Yuen, J. C. (2005). Le regole terapeutiche: L’azione intrinseca dei punti in
Simongini, E. and Bultrini, L. (eds.) Le Lezioni di Jeffrey Yuen - Volume V.
Rome: AMSA.
ejom
e erapeutic Role of the Practitioner’s Heart in Classical Chinese Medicine and Modern Medical Science
Stéphane Espinosa